Protein-energy malnutrition is an energy deficit because of deficiency of all macronutrients. It commonly includes deficiencies of many micronutrients. PEM are often abrupt and total (starvation) or gradual. Severity ranges from sub clinical deficiencies to obvious wasting (with dropsy, hair loss, and skin atrophy) to starvation. Multiple organ systems are often impaired.
Classification and Etiology
PEM may be
•Primary: Caused by inadequate nutrient intake.
•Secondary: Results from disorders or medication that interfere with nutrient use.
Primary PEM
Primary PEM appears mostly in children and the elders who are lacking access to nutrients. PEM can also result from fasting or anorexia nervosa. Child or elder abuse may be a cause.
In kids, chronic primary PEM has two common forms:
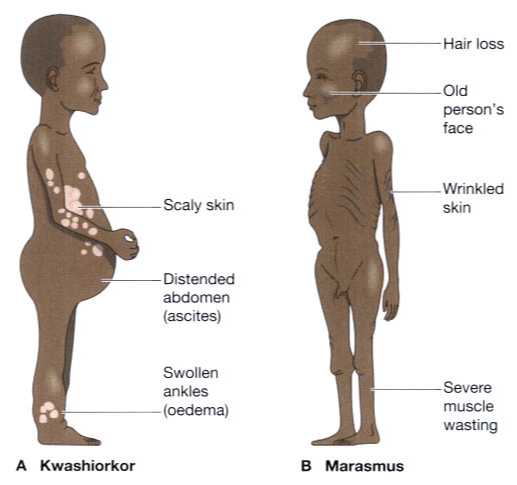
•Marasmus
•Kwashiorkor
The form depends on the balance of nonprotein and protein sources of energy. Starvation is an acute severe style of primary PEM.
Marasmus (also known as the dry style of PEM) causes weight loss and depletion of fat and muscle.
Kwashiorkor (also known as the wet, swollen, or unhealthy form) may be a risk when premature abandonment of breastfeeding, which generally happens once a younger sibling, is born, displacing the older child from the breast.
Secondary PEM
This type most commonly results from the following:
•Disorders that have an effect on GI function: These disorders will interfere with digestion (e.g., pancreatic insufficiency). At the very End-stage heart failure can be a reason of cardiac cachexia, a dangerous form of malnutrition; mortality rate is particularly high.
•Conditions that increase metabolic demands: These conditions include infections, hyperthyroidism, pheochromocytoma, other endocrine disorders, burns, trauma, surgery, and other critical illnesses.
Pathophysiology
The initial metabolic response is decreased metabolic rate. The body will most probably break down adipose tissue to supply energy. However, later, once these tissues are depleted, the body may use protein for energy, resulting in a negative nitrogen balance.
Symptoms and Signs
Apathy and irritability are common. The patient is weak, and work capacity decreases. Cognition and sometimes consciousness are impaired. Temporary lactose deficiency and achlorhydria develop. Gonadal tissues atrophy. PEM can cause amenorrhea in women and loss of libido in men and women.
Muscles shrink and bones protrude. The skin becomes skinny, dry, inelastic, pale, and cold. The hair is dry and falls out simply, becoming sparse. Wound healing is impaired. With acute or chronic dangerous PEM, heart size and cardiac output stops responding; pulse slows down and BP falls rapidly. Respiratory rate and vital capacity decrease. Body temperature falls, sometimes contributing to death. Edema, anemia, jaundice, and petechiae can develop. Liver, kidney, or heart failure may occur.
Marasmus in infants results in hunger, loss of weight, growth retardation, and wasting of certain fat muscle. Ribs and facial bones become prominent. Loose, thin skin hangs in folds.
In kwashiorkor the abdomen protrudes because abdominal muscles are weakened, the intestine is distended, the liver enlarges, and ascites is present. The skin is dry, thin, and wrinkled; affected children may be apathetic but become irritable when held. Total starvation is fatal in eight to twelve wk.
Diagnosis
•Diagnosis usually based on history.
•To determine severity: Body mass index (BMI).
•To diagnose complications and consequences: CBC, electrolytes, BUN, glucose, calcium, magnesium, phosphate.